
This page as a pdf file
Using a DiaPort
Lesley Jordan talks about starting on the DiaPort - where the insulin goes straight into you, and not into the fat under your skin
My DSN suggested a pump in August 2002 because of my unpredictable blood glucose levels due to lipohypertrophy. I started pumping in September 2002 and gained the best control I’d had in years. After about a year, I saw signs that the lipo problem was going to become an issue again with my infusion sites. I saw my DSN and tried a few new areas. However, despite rotating infusion sites, some sites felt slightly lumpy beneath the skin, and became less and less reliable. I thus had to avoid these sites. Even after a couple of months of avoiding them, if I went back to them nothing had changed. I could still keep good control, but had fewer and fewer comfortable, reliable infusion sites as time went on.
I asked IP-UK list members for suggestions, and amongst them was the DiaPort. So I telephoned the DSN at the Royal Bournemouth Hospital, where a limited trial of the DiaPort had all but closed down due to lack of uptake and 1 in 3 failure of the port. Joan Everett, the DSN, asked me to get a referral from my usual diabetes care team (in Essex) to Bournemouth, just for the port (that is, not for my ongoing diabetes care). I saw my diabetologist in August 2004, and a letter was sent in September. I saw Joan and Dr David Kerr in November 2004. Dr Kerr agreed that the lipo was the problem, and suggested that the DiaPort could be a solution. He ran through the drawbacks, and Joan gave me the telephone numbers of the other 2 patients who still had a DiaPort, so I could get the patient’s point of view.
Drawbacks
- Risk of site infection
- Risk of blockage
- Risk of peritonitis
Benefits
- Avoids subcutaneous tissue damage
- No skin irritation from nickel or infusion set adhesives
- No needles even when changing the infusion set
- Uptake by hepatic circulation is more like real pancreatic release than via peripheral circulation
- Rapid and reliable effect of insulin (starts after 3 minutes)
I spoke to another DiaPort patient and decided to go ahead.
DiaPort with scar
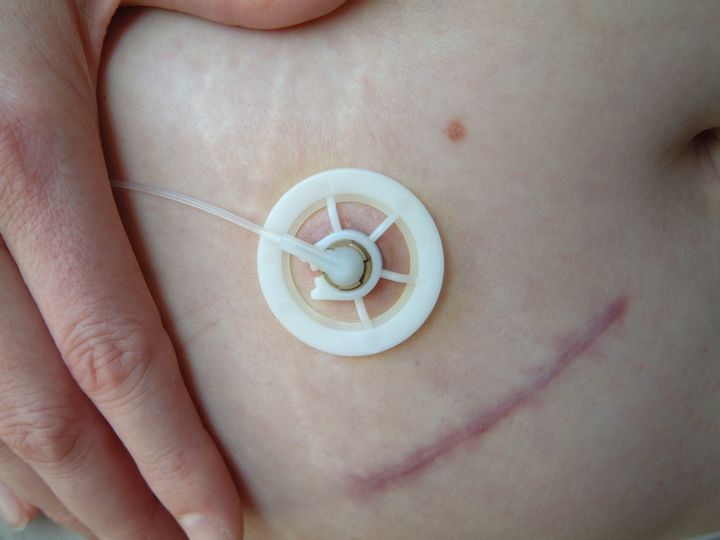
[ Bigger photo ]
The port was inserted under general anaesthetic on 20 December 2004. I had to stay in hospital for 2 nights; the night before and the night after surgery. There were 2 wounds – one where the port pokes through the skin, and another, about 2 inches long, where the surgeon’s fingers did their thing! Infusion was transferred to the port immediately.
Recovery was awful for the first couple of days. I was much more comfortable than I expected to be, and only took paracetamol to kill the pain for a few days. But my blood glucose levels were very difficult to bring down. Although the standard procedure is to reduce the insulin dose by 10%, I needed large correction boluses for the first night, and even a subcut injection when ketones showed up. Eventually Joan and I got it under control and kept it there with a temporary basal rate of around 180%.
DiaPort connection point
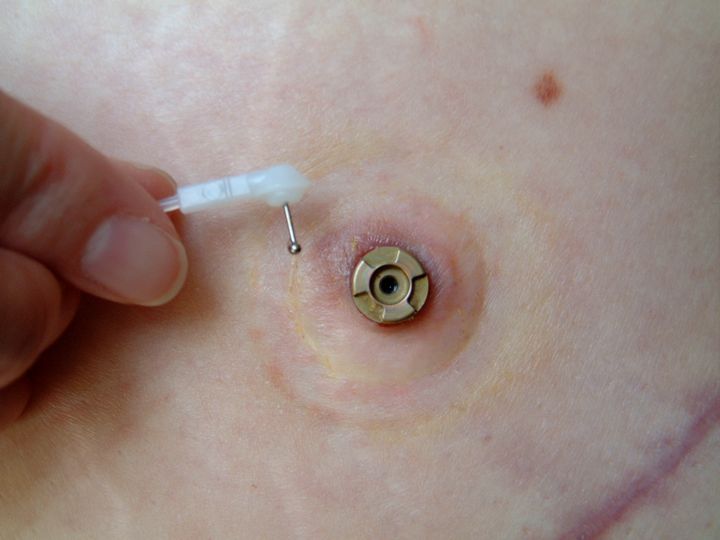
[ Bigger photo ]
The only visible part is a metal bit like the tip of a tube, about half a centimetre high and half a centimetre wide, that pokes through the skin. This is fixed in place with a plastic wheel-like thing, about 2cm diameter, which I have to wear for the first 3 months. There is also a plastic cannula of about 10cm underneath the skin that reaches into my peritoneal cavity. I have to go back to Bournemouth to have the inner catheter changed every 3 months. This will be done within a few minutes by the surgeon, in the day theatre, without any need for anaesthetic.
Daily care was a bit daunting at first, but then so was daily care of the infusion sites when I started pumping. After a month, I didn’t need to wear a wound dressing. Now I just have to clean the area with an alcohol swab every day, and make sure I only handle it with clean hands. But isn’t that the same with subcut infusions?
Using the port has certainly solved the infusion site problems! It’s always in the same spot, and always reliable. Even a big pizza bolus doesn’t sting, and I can change the infusion set last thing at night, if I need to. Such freedom!
I have had one superficial site infection. The area looked red and oozy, and began to itch. My GP gave me a week’s worth of antibiotics and things settled down again.
DiaPort in use
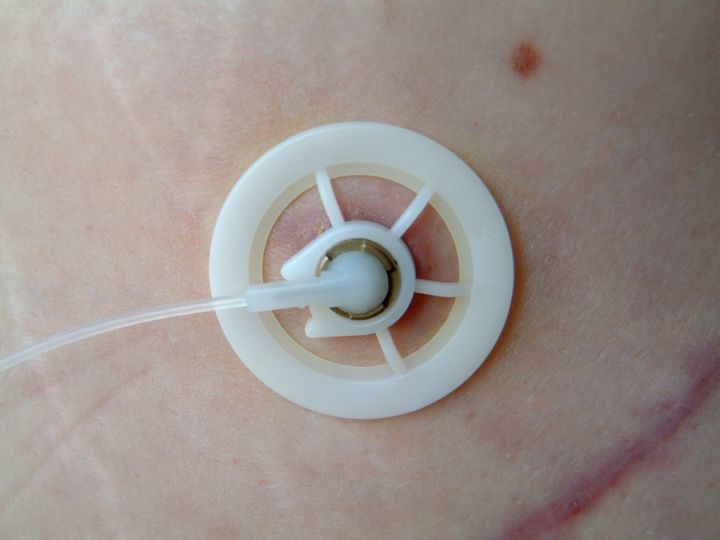
[ Bigger photo ]
The port is very comfortable, I don’t even know it’s there, unlike some infusion sets, which I couldn’t wait to take out after a couple of days. It’s perhaps slightly less discrete than the low profile infusion sets, but it hasn’t been a problem to me.
My only concern now is that I seem to be building up insulin resistance. Prior to the DiaPort insertion, I needed 25 units of basal insulin per day. This has increased to at least 49 units a day, and it seems that every time I need to have a “temporary” basal increase, it doesn’t quite settle back to 100%. So I’m not sure what will happen in the long term.
Apart from that, I’m very happy with the DiaPort, and would recommend it to anyone with ongoing infusion site problems. Those with allergies or needle phobia would also benefit.
Update May 2005: I'm now using 97 basal units per day. My blood glucose levels are often unpredictable, and my daily insulin profile has changed so that my peak insulin delivery is between midday and midnight. This is unacceptable so I have arranged an appointment to discuss this with Dr Kerr - until now, the team seemed uninterested and reluctant to admit this is a problem. However, having agreed to an appointment, they sent one that's only 2 weeks away, which must be pretty good for a busy diabetes outpatient clinic. The protocol for under-delivery shows that an x-ray with radiopaque dye is the next step, to show up any fibrous tissue gathering at the end of the inner catheter. If that's what's causing the problem, then I may need a laparoscopy to clear this tissue.
Update late May 2005: Under general anaesthetic, laparoscopy showed the catheter was completely embedded in the omentum (part of the peritoneum) and surrounded by crystallised insulin. They removed the overgrown omentum and chipped away at the insulin, then inserted a new inner and outer catheter. Time will tell if it will remain clear and function well.
Update July 2005: My basal rates have been increasing steadily again, and another x-ray with dye showed some new crystallisation. At the end of the month I will swap insulin from Humalog to Insuman Infusat, and start flushing with saline every 2 weeks, to try to prevent crystallisation.
Created: Mar 2005; Last updated: Monday 18 July 2005
Reader comments
-
On 29 Jan 2006 Becky wrote:
Hello - I am a 50-year-old Type 1 diabetic, duration 38 yrs. I have had the pump for 6 years. I currently have a site infection and have had one before. I have no insulin resistance, but finding suitable sites for injection is becoming more difficult.
I believe the new inhaled insulin has been approved by the EU, I am in the USA and we should be getting it in June or July. I am looking forward to it.
-
On 17 Aug 2005 Roel Hoogma wrote:
It is not possible to use Humalog for Diaport, because then you will get problems due to chrystallisation. Do only use Insuhuman Ifusat or Regular Insulin, the overgrowth will not respond at saline.
Yours sincerely
Roel Hoogma
Diaport Expert Netherlands -
On 15 Jul 2005 Beryl wrote:
I have Type 2 diabetes and have been using an insulin pump for the last 12 months. I have insulin resistance and using the pump has halved my insulin intake by less than half. I now take 169 units of back ground insulin in twenty four. I used to take over 500 units a day. The problem I have is that I have a plaster allergy and have to change the canula every 12 hours because it gets very sore and itchy. My DSN has clear plastic type dressings to put before I insert the canula. But they make me itchy too. I had never heard of this type of treatment and the way I am looking at things now is that a diaport might be better for me and I am going to mention it at my next appointment with my DSN.
-
On 4 Aug 2005 Lesley replied:
Hi Beryl
It sounds like the Diaport would solve your problem, but unless you are in mainland Europe, it might not be available to you just yet. As far as I know, it's only used in Europe and the very small trial in the UK of which I am a part. So far, the UK trial isn't going very well and has been put on hold. A European clinic which seems to be having great success with the Diaport will publish a paper in the Autumn, so hopefully that will hold the key to the problems we are experiencing in the UK and things will start to move again. I don't think its being trialled in the USA at all.
Best wishes
Lesley
-
On 18 Aug 2005 Beryl replied:
Thanks for your advise. I will mention about the diaport to my DSN and consultant next month, at least then if there are going to be anymore trials in the UK they will know that I am interested and might keep my name in mind if anything does come up. (I come from Liverpool)
-
-